
Over the past year, Health Policy News readers were drawn to topics that were top of mind for many policymakers, as well as articles that detailed innovative solutions to complex problems like controlling health costs and expanding access to healthcare. As 2019 comes to a close, this piece revisits these popular topics, providing updates on recent developments and predictions of what 2020 has in store for these issues including an update on state progress towards a Medicaid Buy-In program; good news out of the state of Connecticut as it partners with Wholesome Wave to bring fresh produce to patients in need; and lastly, a the submission of a concept paper by the state of Vermont to the federal government detailing plans for a state.
Jump to Section:
Medicaid Buy-In Update
Overview
Since 2018, Health Policy News has been tracking the development of Medicaid Buy-In legislation and the release of state studies on these programs. 2019 proved to be an active year for this topic, with the release of fiscal and operational feasibility reports, as well as developments at the legislative level in many states. These developments include the conclusory quantitative report from New Mexico (detailed below) and the passage of Washington state’s SB 5526 – 2019-20 (which directs the state to create a buy-in public option plan utilizing the Washington state-based exchange by 2021).

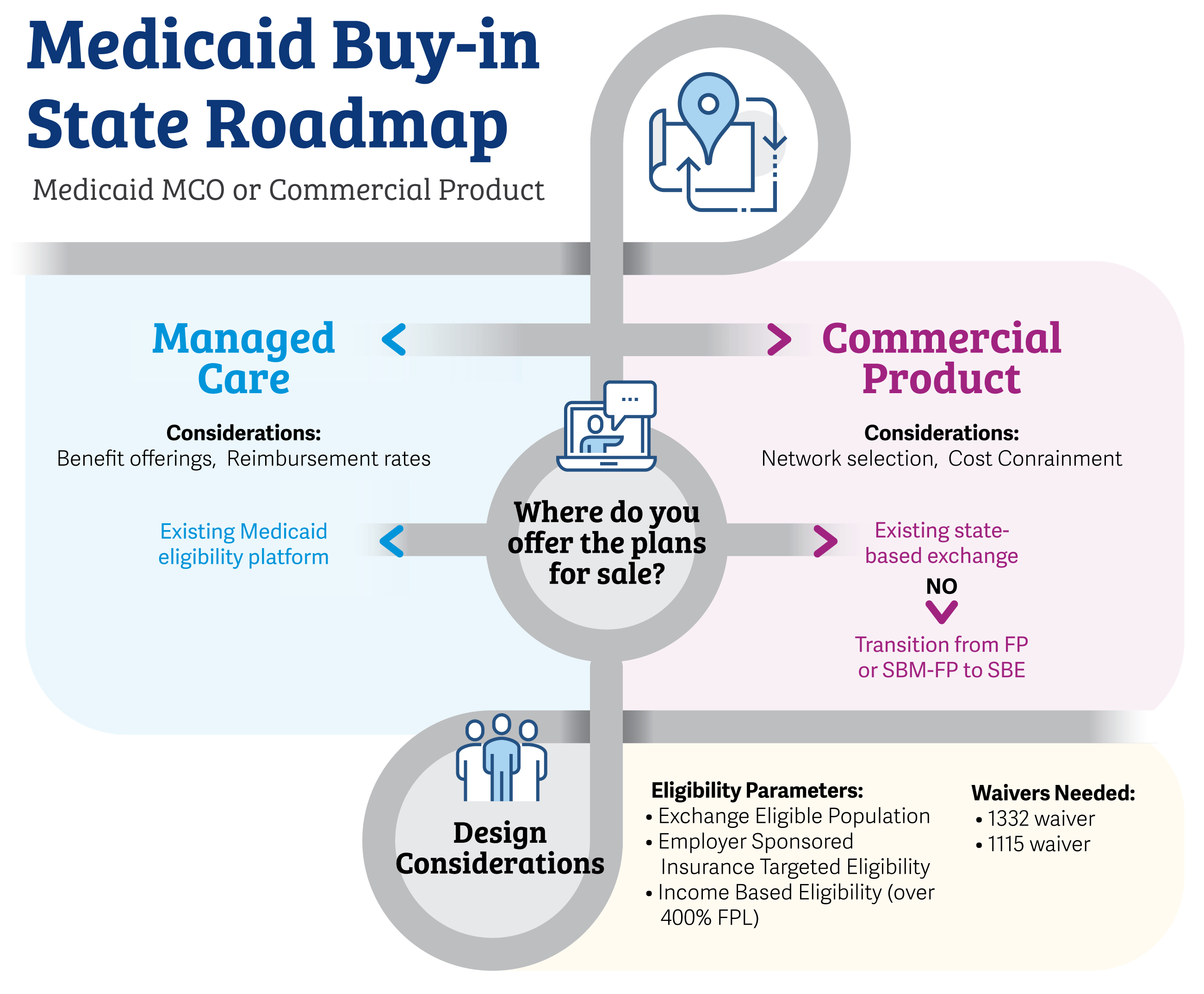
The variety of approaches a state can take to bring about a public insurance product, whether by utilizing commercial or managed care entities, results in a myriad of decision points for policymakers. To assist states in visualizing the options available to them, we have prepared a “Buy-In Roadmap” that highlights some of the key decisions and dependencies in conceptualizing and implementing a buy-in program.
New Mexico Buy-In Activity
Arguably the most comprehensive Medicaid Buy-In feasibility and operational details released to-date are New Mexico’s. Two reports (Phase 1, released December 2018, and Phase 2, released January 2019) issued by the state provide detailed insights for other states about approaches to, as well as potential fiscal and operational considerations for four innovative options. The four models New Mexico considered, which we reported on earlier this year, included:
- Targeted Medicaid Buy-In:New Mexico would offer Medicaid-like coverage off the Marketplace (with the option to subsidize coverage) to those not eligible for Medicaid, Medicare or subsidized Marketplace coverage.
- Low-Cost Marketplace Qualified Health Plan (QHP):New Mexico would offer a lower-cost QHP product on the Marketplace (likely from one existing issuer) to individuals and small employers, with a waiver to ensure affordability and savings.
- Basic Health Plan:New Mexico would create a basic health plan for individuals with incomes up to 200 percent of the federal poverty level (FPL) who are not Medicaid-eligible (including those who are ineligible for Medicaid because of their immigration status)—with an option to expand plan eligibility over time.
- Medicaid for All:New Mexico would allow everyone not otherwise eligible for Medicare to purchase a low-cost health plan option off the Marketplace, with premium subsidy eligibility enrollees applying those subsidies to the purchase of this plan type.
Phase 2 focused specifically on the Targeted Medicaid Buy-In approach—which, as outlined in Phase 1, was presented as the option that would cause the least disruption to the current marketplace. Under this model, the state would provide financial assistance for lower income individuals outside of the Affordable Care Act (ACA) individual market, as well as individuals currently ineligible for Marketplace or other coverage assistance. The state would also provide financial assistance for individuals earning below 200 percent of the FPL who are impacted by immigration status or the “family glitch.”
The state’s Phase 2 report details the following high-level quantitative impacts of the Targeted Medicaid Buy-In option:
- Premiums would be reduced by 15-28 percent relative to the average and lowest-cost premiums in the individual market. Specifically, the buy-in monthly premium would range from $377 to $403 (depending on the buy-in enrollment scenarios)—compared to current estimates of $521 and an estimated lowest-cost premium of $475 for 2020.
- A significant number of individuals would be enrolled in Medicaid. Projected total enrollment for the populations affected (those impacted by immigration status and the family glitch earning up to 200 percent of the FPL, as well as the unsubsidized population) would range from 7,000 to 16,000.
- State costs of providing financial assistance to target groups earning below 200 percent of the FPL would range from $12 million to $48 million, as estimated by Phase 2 modeling results.
This analysis is an important first step in understanding the feasibility of a Medicaid buy-in for New Mexico and should be evaluated as part of a longer-term, comprehensive plan that considers its relationship to other buy-in options, as well as additional state strategies to expand coverage and increase affordability.
 We have also prepared a new tracking chart that details updates from several other key states exploring the idea of a buy-in program (including Massachusetts, Washington, and New Jersey). Click the thumbnail on the left to view this chart. Additionally, for historical insights on the topic of buy-in options, please revisit the white paper and slide deck we prepared as part of our Fall 2018 Policy Webinar Series.
We have also prepared a new tracking chart that details updates from several other key states exploring the idea of a buy-in program (including Massachusetts, Washington, and New Jersey). Click the thumbnail on the left to view this chart. Additionally, for historical insights on the topic of buy-in options, please revisit the white paper and slide deck we prepared as part of our Fall 2018 Policy Webinar Series.
Produce Prescription Program Update
One of our most popular topics in 2019 was the integration of produce prescriptions (produce RXs) into healthcare providers’ toolboxes, as well as efforts to demonstrate the efficacy of these programs. If you missed our previous produce RX coverage, feel free to visit the two articles[1] Health Policy News published concerning increased access to these programs—one of which includes takeaways from an interview we conducted with Wholesome Wave, a leading advocate for produce RX programs.
Wholesome Wave not only champions the importance of access to fresh produce—they provide fresh produce to individuals with food insecurity and diet-related illnesses. As Health Policy News looks back on our 2019 produce RX coverage, we also wanted to update readers on a recent expansion of the Wholesome Wave RX programs: a partnership recently operationalized with Hartford Hospital.
Wholesome Wave kicked off their Connecticut (CT) based initiative this past fall, registering patients through Hartford Hospital to receive up to $60 a month in fresh fruit and vegetable vouchers for use at local stores. The CT program conditions the monthly monetary refill on enrollees meeting certain programmatic requirements tied to the clinical care plan—such as following up with their doctor or attending nutrition counseling. Wholesome Wave calls this three-pronged approach “Inform, Activate, and Measure,” as the refill requirements not only track compliance with purchasing parameters, but also help clinicians understand care compliance incentives and keep in touch with patients to measure health improvements.
As previously mentioned, Wholesome Wave provides tools and guidance for those seeking to establish Produce RX programs. To join their network and take the first step toward increasing access to fresh produce in your area or for your patients, please visit the Wholesome Wave website.
Prescription Drug Importation Update
Closing out this 2019 hot topic retrospective is a prescription drug cost control method that states are pursuing cautiously, eyeing the approaches of early adopter states- prescription drug importation. Just this month, Vermont submitted a report to the federal government outlining the approach and feasibility of allowing state drug importation under certain circumstances, as well as the potential benefits pursuant to federal approval of such a program.
As we previously reported, Vermont passed legislation in May 2018 that allowed the state to apply for federal approval of wholesale importation of certain drugs from Canada. The 2003 Medicare Prescription Drug Improvement and Modernization Act created a pathway for this approach, provided that “implementation of such a program will a.) Pose no additional risk to the public’s health and safety; and b) Result in a significant reduction in the cost of covered products to the American consumer.”[2] In designing prescription drug import programs, states bear the burden of proof for these metrics—and in order to receive approval, must demonstrate to the federal government both the cost savings the program will generate and also the state’s method by which to meet importation safety standards and protocols.
In December 2018, Vermont’s Agency of Human Services (AHS) submitted to the state legislature its proposed program design for the “Canadian Rx Drug Import Supply Program”. This report also provides considerations for next steps in evaluating the program, which include:
- Determining the benefit to Vermonters, including estimates of upfront and ongoing operational costs,
- Outlining the necessary steps to implement the program, including assessing supplier interest.
Vermont’s recent concept paper picks up where their December 2018 program design document left off, detailing how the proposed program will satisfy the federal Food, Drug, and Cosmetic Act (FDCA)’s cost-saving and safety requirements. The report also compares Vermont’s proposed importation program to those under review in other states, including the Florida model—e.g., while Florida’s program is limited to public payors, Vermont’s targets commercial carriers. Readers interested in further highlights from the concept paper can find them summarized in the short slide deck the state released in November 2019.
Health Policy News will continue to follow this topic in 2020, so stay tuned for more insights into developments at the state (and possibly federal) level as policymakers aim to save on prescription drug costs via importation.
Footnotes:
[1] “Eat Your Veggies!” – May 2019 (read here); “How Can Communities Support Fresh Produce Programs for Their Citizens?” – July 2019 (read here)
[2] 21 U.S.C. 5 384
Leave a Reply