



Draft Marketplace Rules & Guidance for Health Issuers
On December 12, 2022, the Department of Health and Human Services (HHS) released the Proposed Notice of Benefit and Payment Parameters for 2024 (NBPP) and the Draft 2024 Letter to Issuers in the Federally-facilitated Exchanges (Letter), along with the below accompanying technical guidance:
- Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage for the 2024 Benefit Year
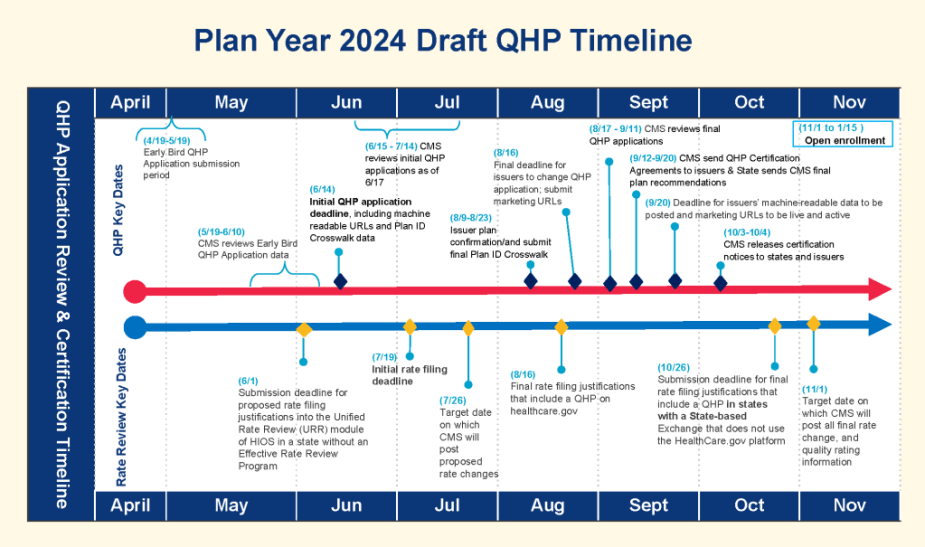
- Proposed Key Dates for 2023 QHP Certification & Rate Review
- Draft 2024 Actuarial Value Calculator
- Draft 2024 Actuarial Value Calculator Methodology
- Proposed QHP Data Submission Certification Timeline Bulletin
- Proposed Rate Review Timeline Bulletin
As always, the NBPP, Letter, and other guidance address key timelines, certification standards, financial parameters, and operational and technical guidance for Exchanges, Qualified Health Plans (QHPs), and premium stabilization programs. Most of this year’s proposals are more adjustments than the major overhauls we have seen in recent prior years, with more significant policy changes focused on network adequacy and essential community provider standards and categories.
Below, we provide our annual overview of the significant proposed policy changes from previous years’ guidance, with a focus on key payment parameters and changes that impact state insurance markets and regulators.
Timeline

Network Adequacy
For the 2024 plan year, HHS will evaluate all QHPs for compliance with network adequacy standards based on time and distance standards and appointment wait time standards, as outlined in 45 CFR 156.230 and 45 CFR 156.235, including requiring all QHPs (including Stand-Alone Dental Plans) to use a provider network. As was the case last year, HHS will be working more closely with states on network adequacy.
Essential Community Providers (ECPs)
In the Letter and NBPP, the following changes to the ECP categories are proposed for Plan Year 2024:
- To add a new ECP category entitled “Mental Health Facilities” that includes Community Mental Health Centers and Other Mental Health Providers.
- To add a new ECP category entitled “Substance Use Treatment Centers,” moving this provider type from “Other” to their own standalone category.
- To add Rural Emergency Hospitals to the “Other ECPs” category.
These proposed changes would require that issuers offer a contract to at least one ECP in each of the eight ECP categories in each country in the service area. The eight categories proposed for 2024 include: Federally Qualified Health Centers (FQHCs), Ryan White Program Providers, Family Planning Providers, Indian Health Care Providers, Inpatient Hospitals, Substance Use Disorder Treatment Centers, Mental Health Facilities, Other ECP Providers.
Issuers would still have to demonstrate 35 percent provider participation of available ECPs, including write-ins for each plans service area, with an additional proposal for 2024 that would require the 35 percent threshold to also be applied within two of the categories; FQHCs and Family Planning Providers. The full chart of the proposed ECP categories, and provider types is included in the Letter starting on pg. 12 and continuing to 13, as Table 2.1.
Standardized Plans
In the NBPP and Letter, HHS has proposed largely minor updates to Federally-facilitated Exchange (FFE)/State-based Exchange-Federal Platform (SBE-FP) individual market standardized plans for 2024 and future years, with a more significant change to non-standardized plan offerings:
- HHS proposes to eliminate the non-expanded Bronze standardized plan option. The only Bronze standardized plan will be an expanded Bronze plan and the requirement to offer standardized plans will only apply to that plan type in the Bronze level.
- HHS will continue to have standardized plans and require issuers to offer them in the following plan levels: expanded Bronze, Silver, each version of income-based Silver cost-sharing reduction variation, Gold, Platinum. The plan designs for those plans have been updated as specified in the NBPP.
- HHS proposes to continue to include a four-tiered drug benefit in standardized plans and has included more specific standards for what types of drugs should be included in each tier, as well as technical guidance in the Letter (see page 8).
- Other requirements related to standardized plans – including related to the requirement to offer, the two sets of standardized plans and differential display have not changed from 2023.
- In a more significant change, HHS is proposing to limit issuers to offering only two non-standardized plans per network type and metal level in each service area for offerings through Exchanges on the Federal platform (FFEs and SBE-FPs). This is something HHS has flagged previously that it would consider. HHS noted in the preamble to the NBPP that an alternative to this limitation would be adopting new, more stringent meaningful difference standards that would be based on deductible amounts.
Prescription Drugs
HHS has proposed changes to the non-discrimination formulary cost share review tool that will ensure cost sharing is not being used to discourage enrollment of individuals with chronic or high-cost medical conditions. This adverse tiering review tool will focus on the following medical conditions: hepatitis C, human immunodeficiency virus, multiple sclerosis, and rheumatoid arthritis.
Cost Sharing
For 2024, HHS proposes the maximum annual limitation on cost sharing of $9,450 for self-only coverage, $18,900 for other coverage, with the cost sharing reduction plan MOOPs outlined below:


Stand-Alone Dental Plans
As always, HHS has also addressed the cost-sharing limitations for Stand-Alone Dental Plans (SADPs) in the Letter, proposing to increase the MOOP for SADPs to $400 for one child and $800 for two or more children.
In the NBPP as well as the Letter, HHS proposes the following additional changes:
- To require SADP issuer to use the enrollee’s age at the time of issuance or renewal for rating and eligibility purposes.
- To require SADP issuers to submit guaranteed rates through all types of Exchanges rather than allowing estimated rates that enrollees must then confirm.
User Fees
As has been the case in recent years, HHS proposes another slight reduction to user fees for 2024:
- FFE user fee: 2.5 percent in 2024, down from 2.75 in 2023.
- SBE-FP user fee: 2 percent, down from 2.25 in 2023.
Re-Enrollment
In the NBPP, HHS proposes to allow Exchanges to alter the automatic re-enrollment hierarchy that determines what plans individuals who do not make a plan selection are enrolled into such that:
- Individuals who are eligible for cost-sharing reductions in the Silver level can be re-enrolled into a Silver level QHP in the same product and with equal or lower premiums (after factoring in the Advance Premium Tax Credit) instead of a Bronze QHP if stated conditions are met.
- Individuals are re-enrolled into plans with the most similar network to their prior plans, again subject to stated conditions.
HHS is also seeking input on a variety of considerations related to possible future changes to re-enrollment hierarchies.
Special Enrollment Periods
HHS proposes several changes aimed at ensuring access to coverage and maintaining continuous enrollment for consumers. One proposal includes allowing assisters to go door-to-door for enrollment purposes, but additional proposed changes include:
- Beginning 1/1/24, states could have the option to implement a new rule that would apply to consumers losing Medicaid or CHIP (likely tied to the known end of continuous enrollment under the Public Health Emergency) that would give consumer 60 days before, or 90 days after the loss of Medicaid or CHIP to enrollee in a QHP.
- Additionally, states could allow consumers to attest to a known end of Medicaid, CHIP of MEC to offer an earlier coverage effective date to prevent gaps in coverage.
Terminations of Coverage based on Aging Out of Dependent Coverage
HHS currently prohibits issuers from terminating coverage of a dependent when they age out of dependent coverage if that change happens mid-plan year. In the NBPP, it seeks to add that prohibition explicitly to the regulations to confirm that issuers are required to cover dependent young adults until the end of the plan year in which they turn 26.
Exchange Blueprints
HHS proposes to amend the timeline according to which states may transition from either a Federally-facilitated Exchange (FFE) to a State-based Exchange (SBE) or a State-based Exchange on the Federal Platform (SBE-FP) or from a SBE-FP to a SBE. HHS proposes that states will be required to have approval or conditional approval of its Exchange Blueprints at some point prior beginning open enrollment either as an SBE or SBE-FP, with the hopes that the additional flexibility will provide more time for federal and state coordination on the transition.